
I wanted to have more
opportunity to suture so I chose plastics surgery as one of my electives.
Plastics surgery currently has PAs working for them. This was a great
opportunity to witness how PAs function in surgery.
 A
normal day
A
normal day
A
normal day
7:00am – meet with the PAs and determine the OR slate for the day
7:30am – head to the OR and help assist the OR nurses set up the
equipment needed for surgery
8:00am – 5pm – OR assist – It was difficult to do much in the OR as
there were plenty of residents to assist. I did get some good suturing
practice. Practiced some dermal and running stitches
CLINICS: These were fun. They were quick visits and I was able to see the outcomes of the surgical procedures that were done.
WHAT I SAW
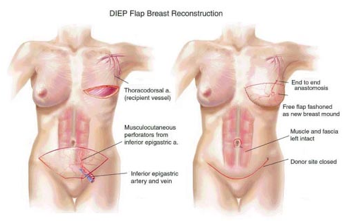
- Mastectomy and breast
reconstruction DIEP method – using abdominal fat to reconstruct the breast and the patient got a free tummy tuck :P. This was amazing.
- Breast lift
- Liposuction
- Scar revision
- Traumatic hand reconstruction
- Flaps
- Latissimus dorsi breast reconstruction
- Carpal tunnel
- Dupuytren contracture
Plastic surgery had more possibilities and depth than I knew coming in. My perceptions of plastic surgery was what I've seen on TV ie. greys anatomy and celebrities. I did not see any cosmetic surgery on this rotation. Most cases were cancer patients that were getting their cancer surgically removed. Plastics was responsible for fixing the area and making it functional. Microsurgery was awe-striking. I never knew such surgery existed. You can literally take any part of your body and attach it somewhere else on your body. Plastic surgery are for those who are detailed orientated as it requires a lot of time and patience to attach small arteries, veins and ligaments.
- Breast lift
- Liposuction
- Scar revision
- Traumatic hand reconstruction
- Flaps
- Latissimus dorsi breast reconstruction
- Carpal tunnel
- Dupuytren contracture
Plastic surgery had more possibilities and depth than I knew coming in. My perceptions of plastic surgery was what I've seen on TV ie. greys anatomy and celebrities. I did not see any cosmetic surgery on this rotation. Most cases were cancer patients that were getting their cancer surgically removed. Plastics was responsible for fixing the area and making it functional. Microsurgery was awe-striking. I never knew such surgery existed. You can literally take any part of your body and attach it somewhere else on your body. Plastic surgery are for those who are detailed orientated as it requires a lot of time and patience to attach small arteries, veins and ligaments.
 |
| Picture I found on the internet- microsurgery |
I was amazed at what the
PAs got to do. One PA who has been working for only 2 years was cutting,
suturing on their own and was well respected by the residents. I could see the
trust the surgeons have with the PAs. They prefer the PA in
assisting in certain cases especially the PAs who have been working there for years. The PAs truly function as
physician extenders. Here they were like residents that never leave. I
recommend this elective for those who are interested in surgery. I
admit it was difficult standing for more than 2 hours, my hips would start
acting up :P . Some cases we would stand even up to 7 hours.
This was a great rotation with awesome PA mentors.
This was a great rotation with awesome PA mentors.




